


How Scaling Up Clinical Research In Africa Can Benefit Society And The Economy
Demographic trends define Africa as the world’s fastest-growing region, with its population potentially doubling by 2050. As the continent achieves significant progress in the control of infectious diseases, the rise of non-communicable conditions, in parallel with the possibility of emerging pandemic pathogens, is adding more pressure to already strained healthcare systems and posing challenges to continental development ambitions.
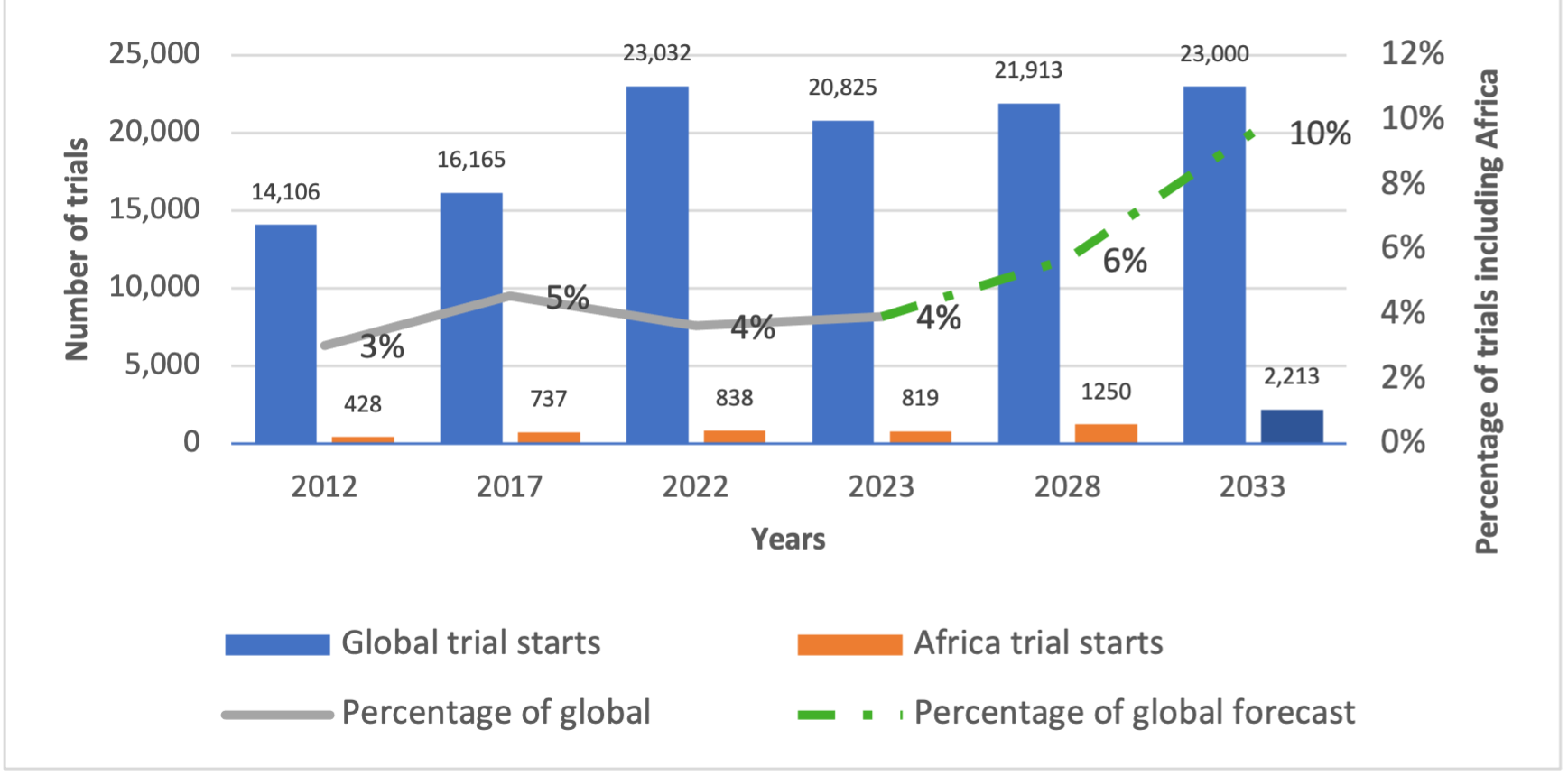
According to IQVIA, out of the 20,825 trials that started globally in 2023, only 819 – or 4% of the total – were hosted by African countries, which resulted in the continent providing less than 2% of genetic data analyzed in genomics research. Most of these trials were not only focused on infectious diseases but also restricted to phases III and IV (or phases focused on comparisons to current treatment standards and long-term effects), remaining consistent with clinical research trends over the last 15 years.
Figure 1 (below) illustrates these dynamics and the scenarios that Africa’s ambition could aspire to.
What if 10% of global clinical trials included African patients? Is this a possibility based on industry growth prospects, especially from the emerging biopharma sector, and what would the benefits be to patients, healthcare systems, and economies?

Figure 1. Clinical trials in Africa versus the rest of the world. Source: IQVIA Global Site Management (2024).
While issues of genomic representation and pandemic preparedness are certainly critical for discoveries, why should we continue insisting on the need to increase investment in African clinical development?
The case for investing in clinical research in Africa
Clinical development has an overwhelmingly positive impact on patient populations in Africa, providing early access to cutting-edge treatments and immunization tools.
Similarly, producing therapies and vaccines that respond better to the genetic and phenotypic specificities of African populations can contribute to improved health outcomes for those living on the continent and the African diaspora migrating to other regions. Clinical trials are also a fundamental resource for global health security, assisting the swift development of vaccines in response to disease outbreaks.
Clinical research can develop or reinforce the medical infrastructure of host countries by increasing access to more global standards of care and directing clinical trial-related fees to hospitals and other sites. This attracts and retains researchers and sets the foundations for future studies. Increasing local research and home-grown innovation also gives way to cost-effective approaches to managing public health priorities, as domestic experiences can guide more targeted interventions.
The uses of trial-generated data can equally strengthen and harmonize regulatory frameworks, persuading life sciences companies to partake in regionalized manufacturing. If increased production can improve the availability of medicines and vaccines and make them more affordable, then additional investments in clinical research in Africa are pivotal to advance equity in access, create economies of scale, and support the inclusion of much-needed therapies in national health insurance schemes.
Studies show that every dollar invested in clinical research has a return of $405 in wider societal and economic gains, with product development in Africa, based on local trials, averting nearly 600 million disability-adjusted life years (DALY) between 2000 and 2022. For example, clinical studies to assess the treatment of schizophrenia with paliperidone palmitate in Rwanda were pivotal to catalysing research and development in other mental health areas, empowering local talent, strengthening local health systems, and adequately engaging patient communities.

{kind=link}
The health problem is simple. The populace in African can use to have better trials and studies based on is populace who have genetic specifics that did and will yield different results in any trial in comparison to other populaces in humanity.
The fiscal problem is also simple. The African continent doesn’t have firms or governments with the money to invest in research and trials expansive enough for the problem stated above.
Engineering is a process, it isn’t a matter of going to school in beijing/new york city/london today and having access to wealthy countries research facilities and going back to africa and waving a magic wand. You have to slowly build the infrastructure in africa itself.
Before the lambourghini, the mercedes motorwagen, before the mercedes motorwagen the carriage, before the carriage the wheel.
To that end, only one organization in Africa has a pan african position in its very legal framework and that is the organization of african unity, so the AU former OAU , needs to be the pathway. In that way the members of the AU need to put monies together and make a clinical trial organization.